Abstract and Introduction
Abstract
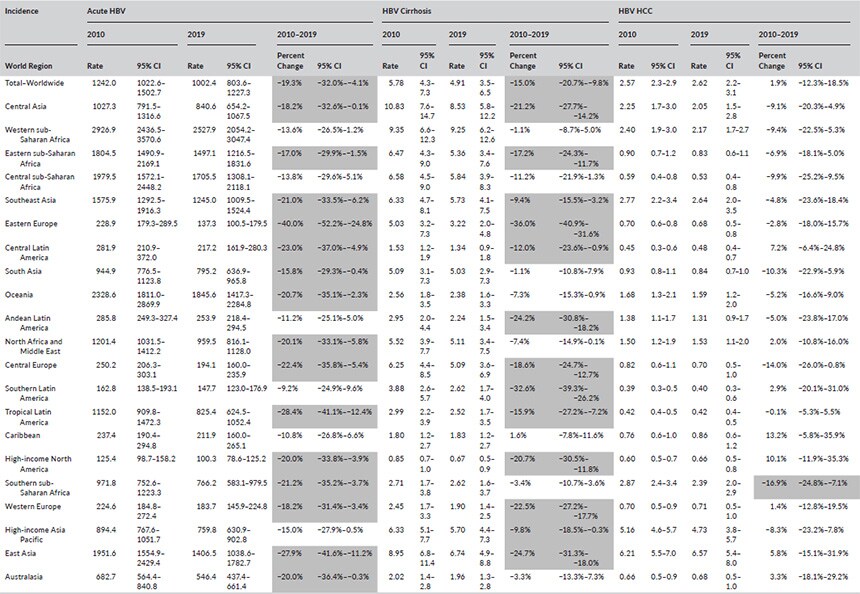
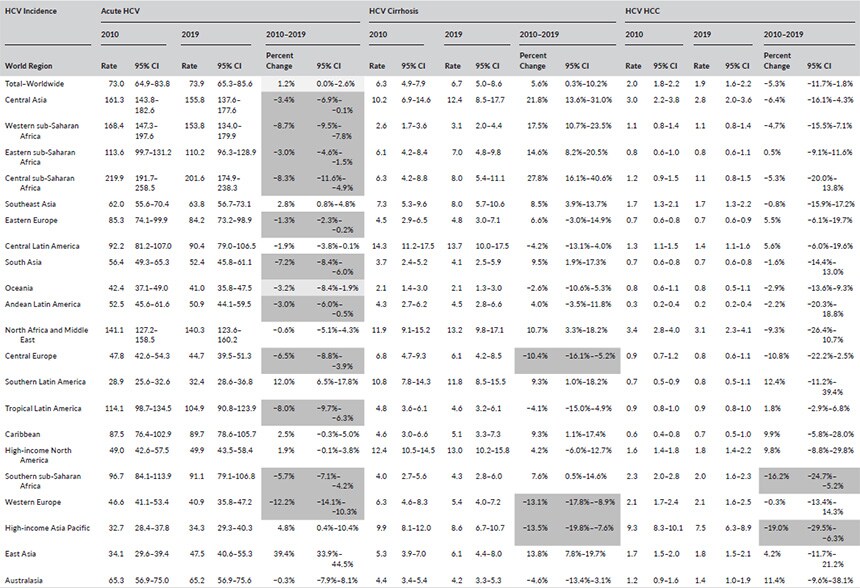
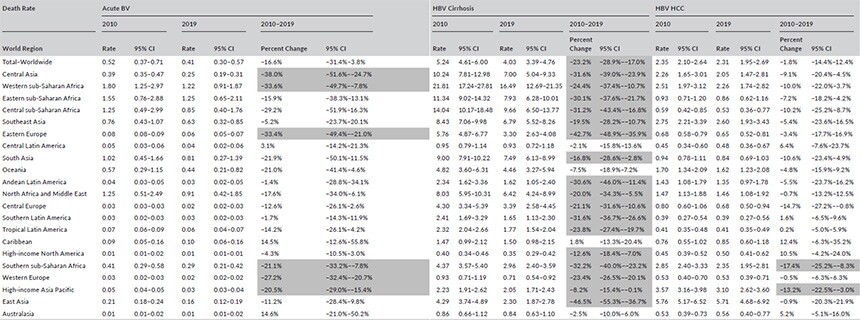
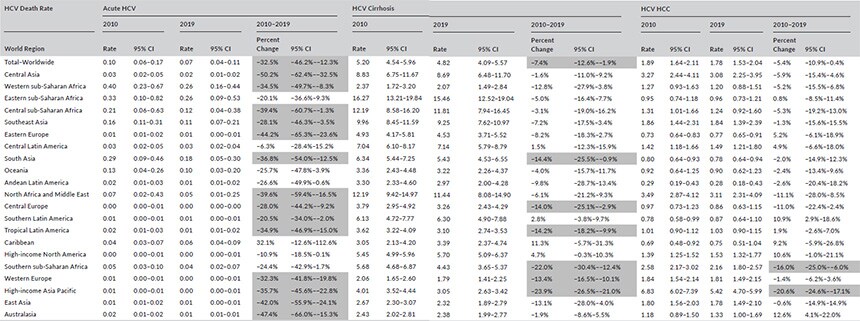
Hepatitis B virus (HBV) and hepatitis C virus (HCV) contribute to significant healthcare burden globally. We aim to provide an updated and comprehensive analysis of global trends in the incidence and mortality of HBV and HCV related acute infections, cirrhosis and hepatocellular carcinoma (HCC). Estimates of annual cause-specific disease incidence and mortality for HBV and HCV were analysed using the 2010–2019 Global Burden of Diseases, Injuries and Risk Factors Study database. Three distinct disease states were evaluated: acute infections, cirrhosis and HCC. Age-standardized disease incidence and mortality were presented per 100,000 population and stratified by age, sex, year and 21 world regions. From 2010 to 2019, overall incidence of acute HBV declined by 19.3% (95% CI 4.1–32.0, p < .05) and HBV cirrhosis declined by 15.0% (95% CI 9.8–20.7, p < .05). Incidence of HCV cirrhosis increased by 5.6% (95% CI 0.3–10.2, p< .05) and HCV HCC remained stable. Incidence of acute HCV declined until 2015, after which it began increasing. From 2010 to 2019, overall mortality for HBV cirrhosis and HCV cirrhosis declined, whereas mortality for acute infections and HCC remained stable. Major differences in HBV and HCV incidence and mortality trends were observed when stratified by world regions. In conclusion, while our analyses of global trends in HBV and HCV incidence and mortality demonstrate encouraging trends, disparities in disease epidemiology were observed across world regions. These observations will identify regions and populations where greater focus and resources are needed to continue progressing towards viral hepatitis elimination.