Abstract and Introduction
Abstract
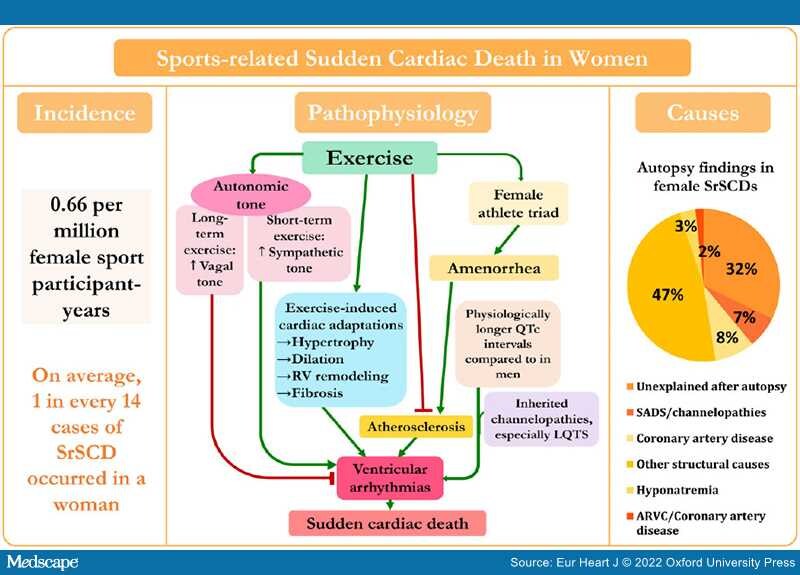
Graphical Abstract

Diagram of incidence, pathophysiology, and causes of sports-related sudden cardiac death in women. The pie chart shows causes of 59 sports-related sudden cardiac deaths in women based on reported data from different studies.[7–9,23,24,26,27,29,38] SADS, sudden arrhythmic death syndrome; RV, right ventricular; LQTS, long QT syndrome; ARVC, arrhythmogenic right ventricular cardiomyopathy. ‡The primary autopsy finding and stated cause of death in one of the hyponatraemia cases was hyponatraemia, yet additional clinical and autopsy data also showed the presence of myxomatous polyvalvular (mitral, tricuspid, aortic) heart disease.
Sudden cardiac death (SCD) is a tragic incident accountable for up to 50% of deaths from cardiovascular disease. Sports-related SCD (SrSCD) is a phenomenon which has previously been associated with both competitive and recreational sport activities. SrSCD has been found to occur 5–33-fold less frequently in women than in men, and the sex difference persists despite a rapid increase in female participation in sports. Establishing the reasons behind this difference could pinpoint targets for improved prevention of SrSCD. Therefore, this review summarizes existing knowledge on epidemiology, characteristics, and causes of SrSCD in females, and elaborates on proposed mechanisms behind the sex differences. Although literature concerning the aetiology of SrSCD in females is limited, proposed mechanisms include sex-specific variations in hormones, blood pressure, autonomic tone, and the presentation of acute coronary syndromes.