Abstract and Introduction
Introduction
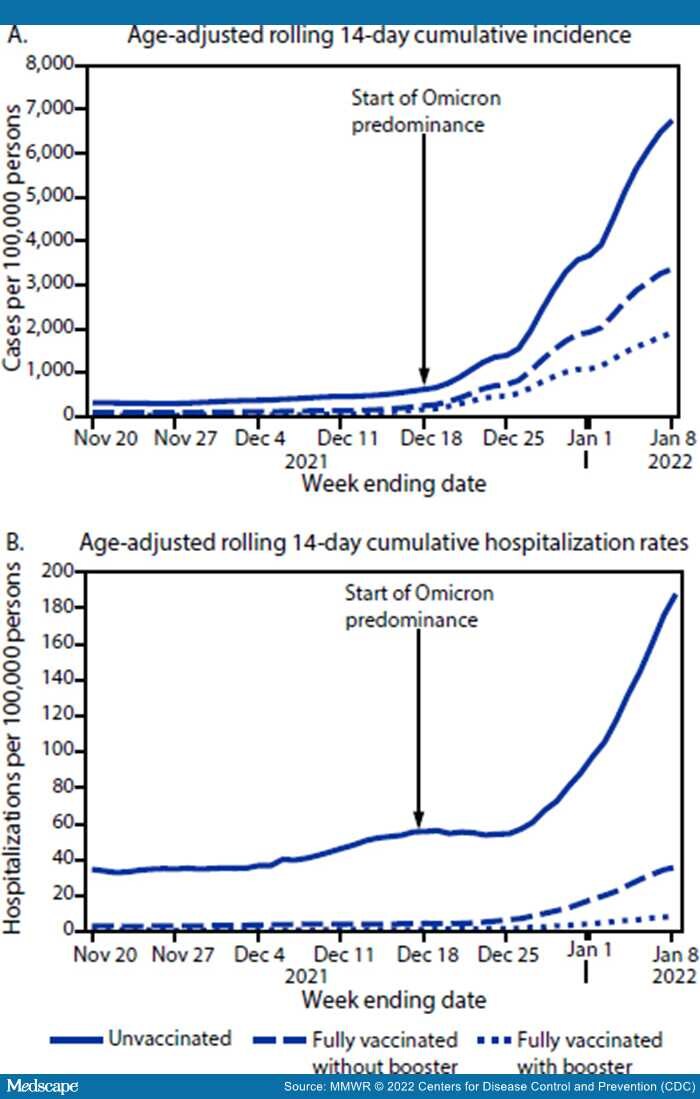
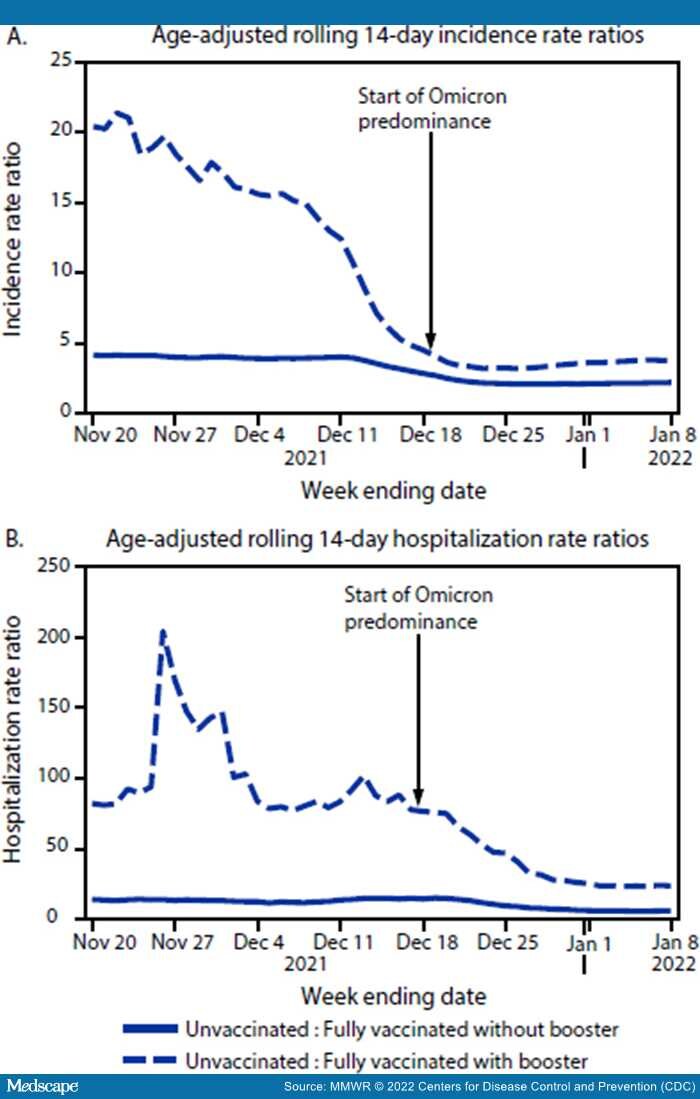
COVID-19 vaccines are effective at preventing infection with SARS-CoV-2, the virus that causes COVID-19, as well as severe COVID-19–associated outcomes in real-world conditions.[1,2] The risks for SARS-CoV-2 infection and COVID-19–associated hospitalization are lower among fully vaccinated than among unvaccinated persons; this reduction is even more pronounced among those who have received additional or booster doses (boosters).[3,4] Although the B.1.1.529 (Omicron) variant spreads more rapidly than did earlier SARS-CoV-2 variants, recent studies suggest that disease severity is lower for Omicron compared with that associated with the B.1.617.2 (Delta) variant; but the high volume of infections is straining the health care system more than did previous waves*,†.[5]The Los Angeles County (LAC) Department of Public Health (LACDPH) used COVID-19 surveillance and California Immunization Registry 2 (CAIR2) data to describe age-adjusted 14-day cumulative incidence and hospitalization rates during November 7, 2021–January 8, 2022, by COVID-19 vaccination status and variant predominance. For the 14-day period ending December 11, 2021, the last week of Delta predominance, the incidence and hospitalization rates among unvaccinated persons were 12.3 and 83.0 times, respectively, those of fully vaccinated persons with a booster and 3.8 and 12.9 times, respectively, those of fully vaccinated persons without a booster. These rate ratios were lower during Omicron predominance (week ending January 8, 2022), with unvaccinated persons having infection and hospitalization rates 3.6 and 23.0 times, respectively, those of fully vaccinated persons with a booster and 2.0 and 5.3 times, respectively, those of fully vaccinated persons without a booster. In addition, during the entire analytic period, admission to intensive care units (ICUs), intubation for mechanical ventilation, and death were more likely to occur among unvaccinated persons than among fully vaccinated persons without or with a booster (p<0.001). Incidence and hospitalization rates were consistently highest for unvaccinated persons and lowest for fully vaccinated persons with a booster. Being up to date with COVID-19 vaccination is critical to protecting against SARS-CoV-2 infection and associated hospitalization.