This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
Imagine that you are unvaccinated, 45 years old, and otherwise healthy. Recently, you spent more than 10 minutes less than 6 feet apart from someone who turned out to have COVID. Currently, you are feeling sick with a cough, fever, and muscle aches. You've also lost your sense of smell.
But here's the wrinkle. You take a rapid, at-home COVID test, and it comes back negative.

What do you do?
That very question was put to 338 individuals in this week's study, appearing in JAMA Internal Medicine.
It's an important question. With free test kits being sent to millions of homes around the country, and with the Biden administration committing to get more home tests onto store shelves, there's about to be a lot more home testing. And that means people need to know what to do with the results.
Now, for our hypothetical scenario — an unvaccinated individual with a recent, close COVID contact who has symptoms consistent with COVID — the recommendations are quite clear: Quarantine, regardless of what the rapid test says, and get yourself a PCR test.
How would the survey respondents, 64% of whom had college educations by the way, fare?
Not too great.
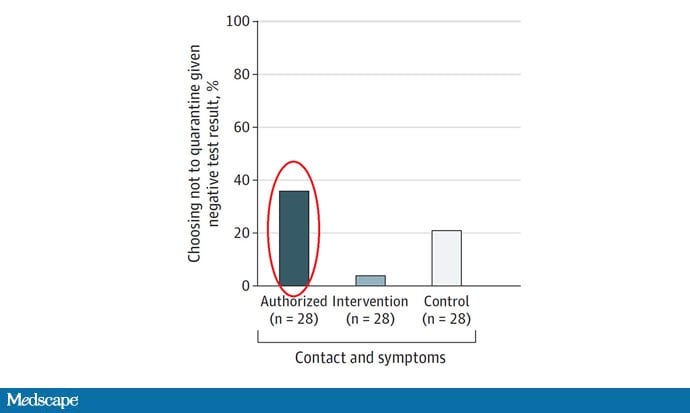
Those who were assigned to read the FDA-authorized instructions included with the Ellume at-home COVID test got the answer wrong 36% of the time.
And when you look at those instructions, you can see why.

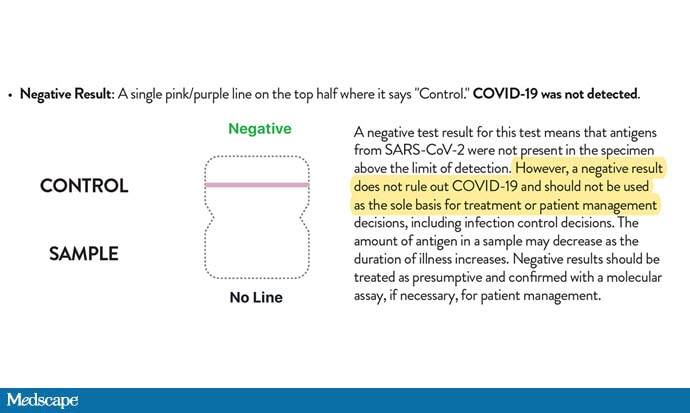
If your test is negative, the authorized instructions say, you are unlikely to have COVID-19 but may have had it previously, and you could get an antibody test to figure that out.
This is just not correct. In fact, while the rapid tests continue to be able to detect Omicron, there are convincing data to suggest that the tests turn positive later in the course of disease than with prior variants.
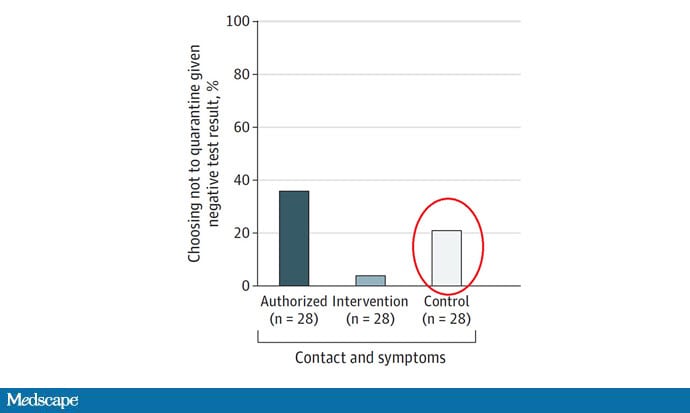
In fact, this language might be worse than no instructions at all. Among individuals presented with no information on how to interpret the tests, only 21% got it wrong.
The authors also provided a third option: an information sheet designed with decision theory principles in mind that makes it very clear what to do with a negative test based on whether you've had a COVID exposure, and whether you've had symptoms.

Just 4% of folks got the decision to quarantine wrong when presented with this enhanced set of patient instructions.
Some good news: There wasn't much confusion after a positive test — everyone knew they should isolate regardless of the instructions they were presented. But this study raises a real concern for an off-target effect of the "tests for everyone" program — false reassurance.
Understanding how to interpret any medical test requires knowing two things: how sensitive the test is at detecting the disease of interest, and how likely you were to have the disease before you tested (the pretest probability). When the pretest probability is high, negative results need to be taken with a large grain of salt, particularly if the test of interest might not be perfectly sensitive.
Sensitivity of at-home COVID tests are quite variable, and more so for Omicron, as this preprint shows.

The FDA acknowledged the reduced sensitivity of antigen tests in the face of Omicron in a December statement, recommending that, among those with symptoms of COVID, a negative home test should be followed by a definitive PCR test.
In other words, if it looks like COVID and sounds like COVID, treat it as COVID — regardless of what a line on a piece of cardboard says.
What this means is that in the coming weeks, more and more people will be testing themselves for COVID. Those that test positive generally know what to do. Those that test negative may not. Healthcare providers need to get the word out that these home tests are great as an initial screen, or to use as a check before visiting a high-risk individual, but PCR tests are better if you have new symptoms. Patient instructions of the type that the authors designed here might go a long way to get that message out.
To be fair, not all home tests do as bad a job of explaining the meaning of a negative test as the Ellume instructions do. The FDA-authorized instructions for the BinaxNow test and the iHealth Covid test — which seems to be the one many people have received in the mail — clearly state that you may still be infectious if you have a negative test.
All in all, I think it's a great thing that we are getting tests into the hands of more people. Knowledge is power. It just might take a modicum of effort, or better design of instructional cards, to teach everyone how to use that power wisely.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale's Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com.
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Credits:
Image 1: Wikimedia Commons
Image 2: JAMA Internal Medicine
Image 3: US Food and Drug Administration
Image 4: JAMA Internal Medicine
Image 5: JAMA Internal Medicine
Image 6: medRxiv
Image 7: US Food and Drug Administration
Medscape © 2022 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: F. Perry Wilson. 1 in 3 People Misinterpret Home COVID Tests - Medscape - Jan 31, 2022.












Comments