This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to another episode of The Curbsiders. I'm Dr Matthew Frank Watto here with my good friend, Dr Paul Nelson Williams. He's going to tell you what we're going to be discussing tonight because we have some great clinical pearls coming your way.
Paul N. Williams, MD: As a reminder, we are an internal medicine podcast. In this video, we will be recapping an interview with the great Dr Michael Barry of the USPSTF about the updated colorectal cancer (CRC) screening guidelines, which are really practice-changing and kind of exciting to talk about. What did you think was one of the most significant and important changes?
Watto: The big news is that the screening age was lowered from age 50 down to age 45. That was given a Grade B recommendation. As a reminder, anything with an A or a B recommendation from the USPSTF is pretty much a preventive service that will be covered by insurance and should be pursued.
This change came about because younger and younger people have been getting CRC, and about 10.5% of new CRC cases are in patients under 50 years old. Patients have been ready for this, having heard about the death of actor Chadwick Boseman (of the Black Panther film) at age 43. Many of my patients, especially young men in their 40s, are asking when they will begin undergoing colonoscopy. But Paul, is it true that you have to have a colonoscopy to screen for CRC? How good are the other tests we have now? There are so many options.
Williams: The great news is that it's not entirely up to you. The nice thing about the recommendation is that USPSTF is relatively agnostic about which screening modality you should use. Direct visualization with colonoscopy is probably still the most sensitive test, but there isn't enough evidence that screening method makes a difference in terms of outcomes.
The best test for your patient is, happily, the test that they're willing to take. If they prefer colonoscopy, terrific. A big factor in choosing a screening method is screening intervals for that method. If results of the colonoscopy are stone-cold normal, that's 10 years until their next colonoscopy. If patients feel that colonoscopy is too invasive, they might prefer to take a stool-based test. Make sure patients are aware that the screening intervals for these tests are much shorter, and if the test results are abnormal, they will still have to undergo a colonoscopy to follow up. Whichever test you can negotiate with your patients and meets their needs is probably the best option.
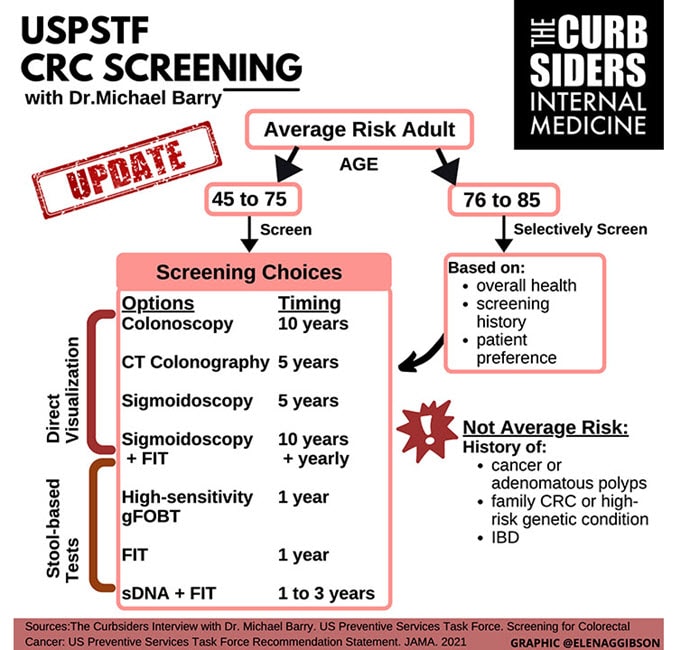
Watto: This graphic, created our great producer, Elena Gibson, really lays it out there for you. The screening interval ranges from 1 to 10 years, depending on screening test. The key point is that colonoscopy, sigmoidoscopy, or stool-based tests lower CRC incidence and mortality to a significant degree. It's not controversial that screening for CRC is effective. This has really changed my practice because I was primarily trying to get patients to have colonoscopies. Some people need to take a day off from work for a colonoscopy and arrange transportation home if anesthesia is used.
It's a big deal for some patients, and some may prefer a stool-based test. The fecal immunochemical test (FIT) analyzes blood in the stool. It's a new-age test that doesn't require the dietary limitations associated with older guaiac tests. They just have to collect a stool sample, something that some of my patients have trouble with and must make two or three attempts before they get the hang of it. The DNA FIT test is a bit fancier. The patient has to collect an entire bowel movement, and the screening interval is 1-3 years.
I was excited about the recommendation that patients now have so many choices for CRC screening. Hopefully this will capture many patients who have resisted colonoscopy in the past.
Williams: With so many CRC screening methods, I'm seeing more enthusiasm for CRC screening, even among older patients, and not just the younger patients we are reaching out to. Patients across the board are much more willing to undergo screening since this new recommendation was made.
Watto: What about the patient between 75 and 85 years old? I know that you and I have a pretty similar practice on this. How should we handle CRC screening in this age group?
Williams: I like how personalized these recommendations are; they aren't quite so boilerplate. The long and short of it is, have a discussion with patients about their preferences. You can consider offering screening to patients between the ages of 75 and 85, depending on comorbidities and estimated life expectancy. In the past, we have discussed chronological age vs biological age. For someone who is relatively high-functioning and interested in screening, it's perfectly reasonable to have that conversation. But for frail patients with multimorbidity, it's probably not something that has to be the top of your list. Screening is now very personalized and based on your estimation of their risk and the patient's wishes.
Watto: A patient aged 75-85 who has never had a colonoscopy, but has a biological age of 65 years, is still likely to benefit from having their index colonoscopy at that age. And patients who have had normal testing up to that age range are probably in a lower-risk category. If they are still healthy and they might undergo treatment, then it's reasonable to continue. It's very nuanced. In medicine, some patients and some of us would love things to be black and white: Just tell me what to do. But of course, it's never that easy. And that's what makes medicine interesting.
Williams: Sure. This has been another episode of The Curbsiders, giving you a little knowledge food for your brain hole. If you found this topic helpful or you'd like to learn more, just click on the podcast link to read our show notes and listen to the entire podcast episode. Until next time, I've been Dr Paul Nelson Williams.
Watto: And I have been Dr Matthew Frank Watto. Goodnight.
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
© 2021 WebMD, LLC
Cite this: CRC Screening: Which Test Is Best? - Medscape - Oct 19, 2021.












Comments