Abstract and Introduction
Introduction
End-stage renal disease (ESRD) is a condition in which kidney function has permanently declined such that renal replacement therapy* is required to sustain life.[1] The mortality rate for patients with ESRD in the United States has been declining since 2001.[2] However, during the COVID-19 pandemic, ESRD patients are at high risk for COVID-19–associated morbidity and mortality, which is due, in part, to weakened immune systems and presence of multiple comorbidities.[3–5] The ESRD National Coordinating Center (ESRD NCC) supports the Centers for Medicare & Medicaid Services (CMS) and the ESRD Networks†,§ through analysis of data, dissemination of best practices, and creation of educational materials. ESRD NCC analyzed deaths reported to the Consolidated Renal Operations in a Web-Enabled Network (CROWNWeb), a system that facilitates the collection of data and maintenance of information about ESRD patients on chronic dialysis or receiving a kidney transplant who are treated in Medicare-certified dialysis facilities and kidney transplant centers in the United States. Excess death estimates were obtained by comparing observed and predicted monthly numbers of deaths during February 1–August 31, 2020; predicted deaths were modeled based on data from January 1, 2016, through December 31, 2019. The analysis estimated 8.7–12.9 excess deaths per 1,000 ESRD patients, or a total of 6,953–10,316 excess deaths in a population of 798,611 ESRD patients during February 1–August 31, 2020. These findings suggest that deaths among ESRD patients during the early phase of the pandemic exceeded those that would have been expected based on previous years' data. Geographic and temporal patterns of excess mortality, including those among persons with ESRD, should be considered during planning and implementation of interventions, such as COVID-19 vaccination, infection control guidance, and patient education. These findings underscore the importance of data-driven technical assistance and further analyses of the causes and patterns of excess deaths in ESRD patients.
CROWNWeb¶ is the national ESRD patient registry and contains administrative and clinical data submitted by dialysis facilities in the United States.[6] Dialysis facility admission and discharge records in CROWNWeb for transplant and dialysis patients were accessed to identify decedents. Estimates of excess deaths during the early months of the COVID-19 pandemic (February–August 2020) were expressed as a range based on methodology established by CDC.[7] The upper limit of excess deaths was defined as the difference between the observed and the predicted number of deaths; the lower limit was defined as the difference between the observed number of deaths and the upper end of a one-sided 95% prediction interval from the model. The predicted number of deaths was calculated using a Poisson model with five variables: year, month, age group, age-group-by-year interaction term, and ESRD Network service area. The month and year variables were added to model the seasonal and secular trends in mortality, which were observed in the data. The model was fit with observations from 2016 to 2019; predictions for 2020 assume that seasonal and secular trends in death rates observed during 2016–2019 were replicated in 2020.** All analyses were conducted using SAS (version 9.4; SAS Institute). This activity was reviewed by CMS and was conducted consistent with applicable federal law and CMS policy.††
Excess death estimates during February 1–August 31, 2020, at the ESRD Network service area and national levels were compared with the total ESRD patient population size from February 2020 to allow comparisons between populations. Excess mortality for all ESRD patients was compared using analyses that included dialysis or kidney transplant patients, defined by the last treatment type for each patient before death.§§ For each subgroup analysis, a new prediction model was estimated, and the numbers of patients who had a most recent dialysis treatment or kidney transplant before death or before February 1, 2020, were used to calculate the total dialysis or kidney transplant patient population sizes, respectively.
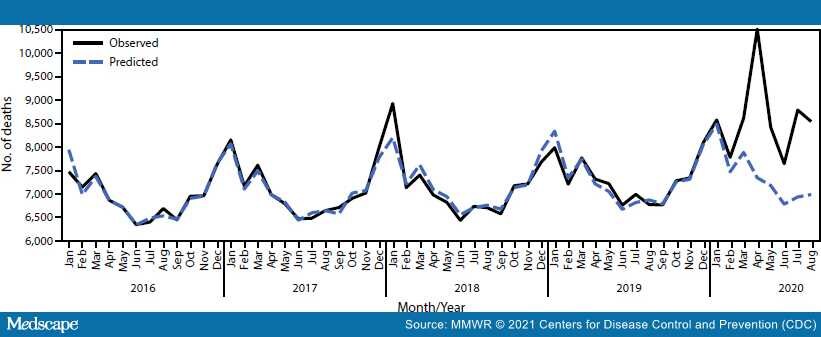
A total of 410,297 decedents were identified in the CROWNWeb data set during January 1, 2016–August 31, 2020, including 60,317 (14.7%) deaths that occurred during February 1–August 31, 2020. Based on the 798,611 patients who were on dialysis or had a kidney transplant as of February 2020, an estimated 8.7–12.9 excess deaths per 1,000 patients occurred among this ESRD population during the early phase of the COVID-19 pandemic, representing 6,953–10,316 excess deaths (Figure 1). Excess deaths at the national level peaked in the early months of the pandemic with a smaller peak in late summer.
Figure 1.
Observed* and predicted† monthly deaths among patients with end-stage renal disease — United States, January 1, 2016–August 31, 2020
Abbreviation: CROWNWeb = Consolidated Renal Operations in a Web-Enabled Network.
*Based on CROWNWeb data from January 1, 2016 through August 31, 2020.
†Based on a model fit with monthly data from January 1, 2016 through December 31, 2019.
For the subgroup analyses of dialysis and transplant patients, as of February 2020, a total of 541,932 dialysis patients and 256,671 transplant patients were identified in CROWNWeb; eight patients were excluded because of missing data. Nationwide, among dialysis patients, an estimated 10.8–16.6 excess deaths per 1,000 patients (5,860–9,019 excess deaths) occurred, and among kidney transplant patients, an estimated 2.6–5.5 excess deaths per 1,000 patients (663–1,403 excess deaths) occurred.
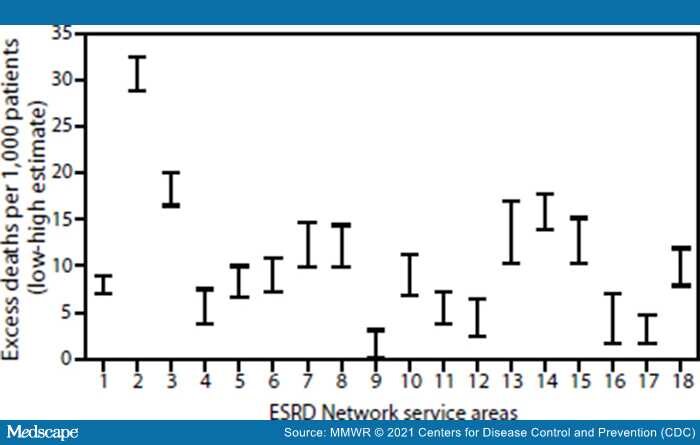
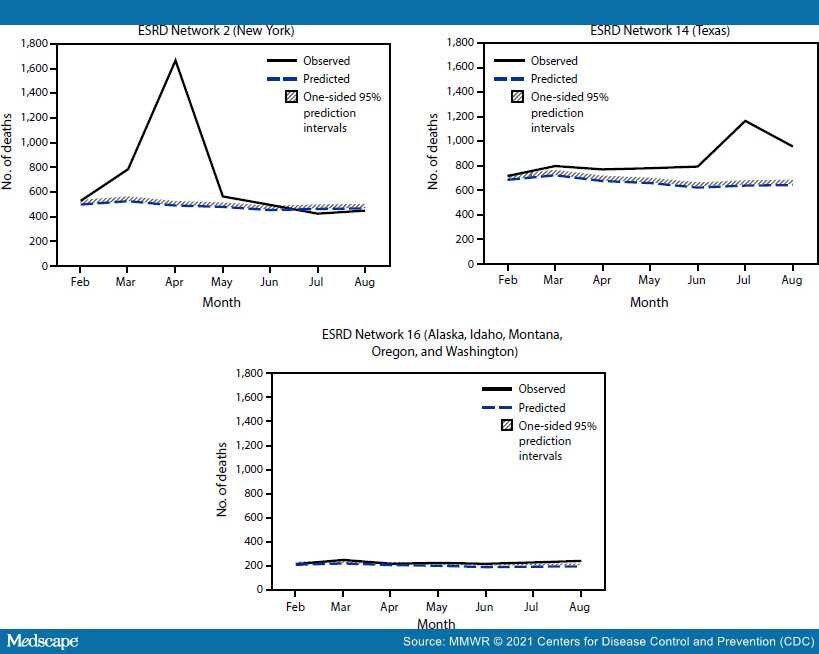
The three ESRD Network service areas with the highest estimated number of excess deaths per 1,000 patients were Network 2 (New York), Network 3 (New Jersey, Puerto Rico, and U.S. Virgin Islands), and Network 14 (Texas) (Figure 2). This is consistent with CDC data indicating that during late January–October 2020, the largest number of COVID-19–associated deaths occurred in California, New Jersey, New York, and Texas¶¶.[8] Substantial variation among ESRD Network service areas in the temporal pattern of excess death was observed. For example, in the Network 2 service area, an increase in excess deaths was observed during March–May; however, very few or none occurred in later months, depending on the estimate (Figure 3). In contrast, in the Network 14 service area, where the initial peak of COVID-19 cases occurred later, excess deaths increased more gradually until July. In some Network service areas, such as Network 16 (Alaska, Idaho, Montana, Oregon, and Washington), few excess deaths were identified over the entire observation period. The observation of fewer excess deaths per 1,000 ESRD patients in regions affected later in the pandemic is consistent with studies of excess deaths in the overall U.S. population.[9]

Figure 2.
Range of high* and low† estimates of excess deaths per 1,000 ESRD patients,§ by ESRD Network service area¶ — United States, February 1–August 31, 2020
Abbreviation: ESRD = end-stage renal disease.
*High estimates were calculated as the difference between the observed number of deaths and the predicted number of deaths from the model, divided by the number of prevalent ESRD patients as of February 1, 2020.
†Low estimates were calculated in a similar manner but used the upper end of the one-sided 95% prediction interval from the model in place of the mean model prediction.
§Networks 2, 3, and 14 had the highest estimated number of excess deaths per 1,000 patients.
¶ Network 1: Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont; Network 2: New York; Network 3: New Jersey, Puerto Rico, and U.S. Virgin Islands; Network 4: Delaware and Pennsylvania; Network 5: District of Columbia, Maryland, Virginia, and West Virginia; Network 6: Georgia, North Carolina, and South Carolina; Network 7: Florida; Network 8: Alabama, Mississippi, and Tennessee; Network 9: Indiana, Kentucky, and Ohio; Network 10: Illinois; Network 11: Michigan, Minnesota, North Dakota, South Dakota, and Wisconsin; Network 12: Iowa, Kansas, Missouri, and Nebraska; Network 13: Arkansas, Louisiana, and Oklahoma; Network 14: Texas; Network 15: Arizona, Colorado, Nevada, New Mexico, Utah, and Wyoming; Network 16: Alaska, Idaho, Montana, Oregon, and Washington; Network 17: American Samoa, Guam, Hawaii, Northern Mariana Islands, and Northern California; Network 18: Southern California.

Figure 3.
Patterns in observed* and predicted† monthly deaths in the ESRD population from selected ESRD Network service areas — United States, February 1, 2020–August 31, 2020
Abbreviations: CROWNWeb = Consolidated Renal Operations in a Web-Enabled Network; ESRD = end-stage renal disease.
*Observed number of monthly deaths was based on CROWNWeb discharge records.
†Predicted number of monthly deaths was based on a model fit with data from 2016–2019. One-sided 95% prediction intervals for the model were also calculated.
Morbidity and Mortality Weekly Report. 2021;70(22):825-829. © 2021 Centers for Disease Control and Prevention (CDC)