In December 2020, the US House of Representatives passed legislation to cover immunosuppressive medications for kidney transplant recipients. Known as H.R. 5534 and S. 3353, the Comprehensive Immunosuppressive Drug Coverage for Kidney Transplant Patients Act of 2020 will provide longer Medicare coverage of these vital medications for our kidney transplant recipients. This bill, along with new therapeutic protocols that identify more efficacious and less toxic induction and maintenance regimens, is geared toward preventing allograft rejection, kidney toxicity, and systemic infection.
Minimizing the risk for each of these events can increase patient and allograft survival. However, there is one modifiable risk factor for allograft failure that has not commanded as much attention from the kidney community: ischemia-reperfusion injury (IRI). IRI is a major determinant of allograft longevity and patient survival. Previously, deceased donor allografts were transported in ice, but today, a cold preservation solution is used. The University of Wisconsin (UW) machine preservation solution is the standard agent used, but it is not perfect, and IRI remains a significant cause of early allograft dysfunction. Oxygenation of the UW solution may further reduce the risk for IRI and extend allograft survival.
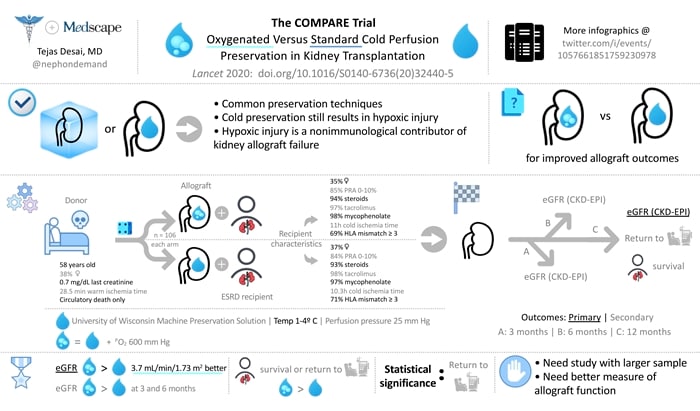
Figure. Download PDF here
The randomized, double-blind COMPARE trial evaluated the effect of supplemental oxygen during hypothermic machine perfusion on kidney transplantation outcomes in kidney pairs from 106 deceased donors who succumbed to circulatory death. One kidney from each pair was randomly assigned to different recipients using (1) the standard UW preservation solution or (2) an oxygenated UW preservation solution. Both are a 1-4° C solution but the oxygenated version is infused with 100% oxygen to achieve a partial pressure (in solution) of 600 mm Hg. The study population included end-stage renal disease patients with near-identical panel reactive antibodies and human leukocyte antigen mismatches. The primary outcome was allograft kidney function at 12 months as measured by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
The results of COMPARE are interesting. Allograft function at 12 months improved by nearly 4 mL/min/1.73 m2 in the oxygenated group, the only endpoint to reach statistical significance. It is somewhat disappointing that none of the secondary endpoints, such as allograft function at 3 and 6 months or patient survival and freedom from dialysis at 12 months, reached statistical significance.
Perhaps this is a result of a small sample size or the use of the CKD-EPI equation to measure allograft function. I wonder what the data would look like if a 24-hour creatinine clearance or cell-free DNA assay had been used instead. I think the data from COMPARE are compelling and warrant further investigation of oxygenated cold preservation solutions, because we desperately need a nonimmunologic tool that can reduce IRI and prolong allograft survival.
Tejas Desai is a practicing nephrologist in Charlotte, North Carolina. His academic interests include the use of social media for physician, student, and patient education. He is the founder of NOD Analytics, a free social media analytics group that serves the medical education community. He has two wonderful children and enjoys spending time with them and his wife.
Follow Tejas P. Desai, MD, on Twitter: @nephondemand
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
- 0
Medscape Nephrology © 2021 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Tejas P. Desai. Do Oxygenated Cold Preservation Solutions Improve Transplant Outcomes? - Medscape - Jan 28, 2021.








