Mineralocorticoid receptor antagonists (MRAs) are still finding their place in nephrology. Many of us relegate them to the bottom of our therapeutic bag for use only after we've exhausted other renin-angiotensin-aldosterone (RAAS)-modifying agents such as angiotensin-converting enzyme inhibitors and/or angiotensin receptor blockers. MRAs target the RAAS axis, and recent trials such as PATHWAY-2 and ReHOT have shown their value, but not as first-line agents. One limitation is hyperkalemia, an adverse effect that not only limits the dose we can use but also frightens many nephrologists away from MRAs altogether.
Recently, a new crop of investigational MRAs has arrived on the scene. Unlike spironolactone and eplerenone, selective MRAs such as esaxerenone and finerenone exert greater antagonism of the mineral receptor.
They have been biochemically engineered to inhibit the RAAS axis without causing dose-limiting hyperkalemia. ESAX-HTN is one of a series of trials looking at the efficacy and safety of selective MRAs, and the results are promising.
It included just over 1000 patients with resistant hypertension from 43 Japanese centers (mean SBP and DBP of 155 and 98 mm Hg, respectively). Patients were randomly assigned to receive eplerenone 50 mg daily or esaxerenone at one of two daily doses (2.5 mg or 5 mg) and were followed for 12 weeks.
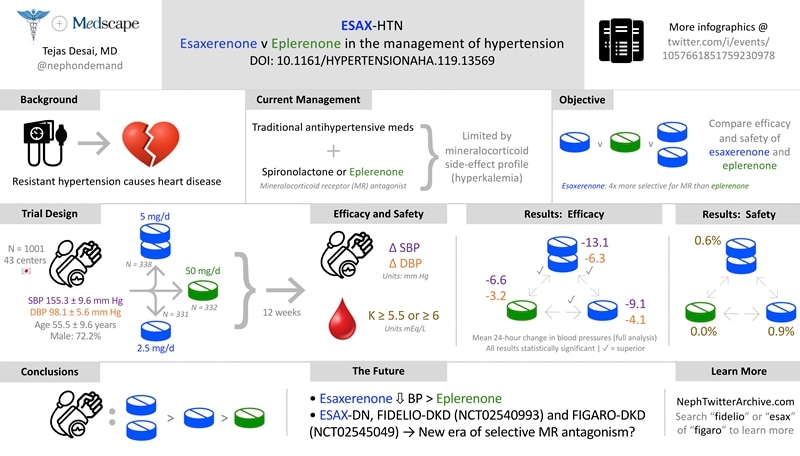
Patients in the high-dose esaxerenone group experienced the greatest drop in both SBP and DBP (decreases of 13.1 and 6.3 mm Hg, respectively). Even those in the low-dose esaxerenone group experienced a larger drop in SBP and DBP than did the eplerenone group. No patients in the eplerenone group experienced hyperkalemia, while less than 1% experienced it in the low- and high-dose esaxerenone groups.
If these selective MRAs can induce similar or greater antihypertensive effects with similar or fewer episodes of hyperkalemia, then we may be more likely to use this class of agents. MRAs may no longer be the third- or fourth-line agent for the treatment of hypertension. With the anticipated publications of ESAX-DN and FIDELIO-DKD and interim data from FIGARO-DKD, selective MRAs may even have an expanded role in combating diabetic kidney disease.
In the meantime, we still have spironolactone and eplerenone at our disposal. Do you use either agent? How do you combat hyperkalemia, and what is/are your thresholds for drug discontinuation? Teach us with your comments below.
Tejas Desai is a practicing nephrologist in Charlotte, North Carolina. His academic interests include the use of social media for physician, student, and patient education. He is the founder of NOD Analytics, a free social media analytics group that serves the medical education community. He has two wonderful children and enjoys spending time with them and his wife.
Follow Tejas P. Desai, MD, on Twitter: @nephondemand
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Medscape Nephrology © 2020 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Tejas P. Desai. Will Mineralocorticoid Receptor Antagonists Move Higher Up the Hypertension Treatment Pathway? - Medscape - Sep 04, 2020.











Comments