
Jaya Mallidi, MD, MHS
"If he were your family member, would you still recommend medical therapy first?" the primary care physician asked with genuine concern over our mutual patient, Mr Simon.*
I had seen Mr Simon for evaluation of chest pain. He was a sturdy man who lived alone with his dog, Midge. His unkempt, long silver beard made him look older than his age of 66 years. For at least 6 months, he has been having chest pain when taking Midge on long walks. He had a stress test 3 days before his visit with me. On treadmill, he walked for 7 minutes, and the imaging study showed a mild area of ischemia in the inferior wall. He had chronic stable angina or stable ischemic heart disease (SIHD).
He was not taking any medications. "I don't like taking pills, and so avoid seeing doctors," he said defiantly. Over the next hour, we discussed his diagnosis, treatment options, and importance of medication compliance. By the end of our conversation, he was willing to take aspirin and beta-blockers. "That's a good start," I said, smiling and advised him to come back to reevaluate in a few weeks.
Two days later, I got the call from his primary care physician asking why coronary angiography was not considered.
COURAGE and Beyond
In patients with SIHD, we know from the landmark COURAGE trial,[1] published more than a decade ago,and meta-analysis of several studies[2] that percutaneous coronary intervention (PCI) plus optimized medical therapy (OMT) compared with OMT alone will not reduce the risk for death or myocardial infarction (MI). PCI may provide more immediate angina relief, but with time, the benefit attenuates.[1] ORBITA,[3] a small, blinded randomized study with a sham-control arm, suggests that the angina relief seen with PCI is largely a placebo effect.
In patients with SIHD, even those with objective evidence of a moderate to large area of ischemia, to date PCI has not been shown to reduce the risk for death or MI definitively. The ongoing ISCHEMIA trial[4] will evaluate this further.
Given the current evidence, various society guidelines support OMT and risk factor management as the first line of therapy in patients with SIHD and no high-risk features on a stress test.[5] A large area of ischemia involving more than one coronary artery territory, left ventricular dysfunction, and dilation of the left ventricular cavity are considered high-risk features on a myocardial perfusion study.[6] Our patient, Mr Simon, had none of these features.
Real-World Practice Paradigm
Despite the existing evidence, in everyday interventional cardiology practice, it is common to get patient referrals from both primary care physicians and general cardiologists for cardiac catheterization and PCI without a trial or even initiation of OMT. Even negative press against stents and interventional cardiologists[7] has not deterred use of the following common practice paradigm in the real world:
Chest pain = stress test
Abnormal stress test result = coronary angiography + possible PCI
Why does such a reflexive paradigm continue in SIHD management? More than the financial incentives associated with doing tests and procedures, it is the "cognitive ease" of such protocolized paradigms that drive these behavioral patterns.
System 1 Versus System 2 Thinking
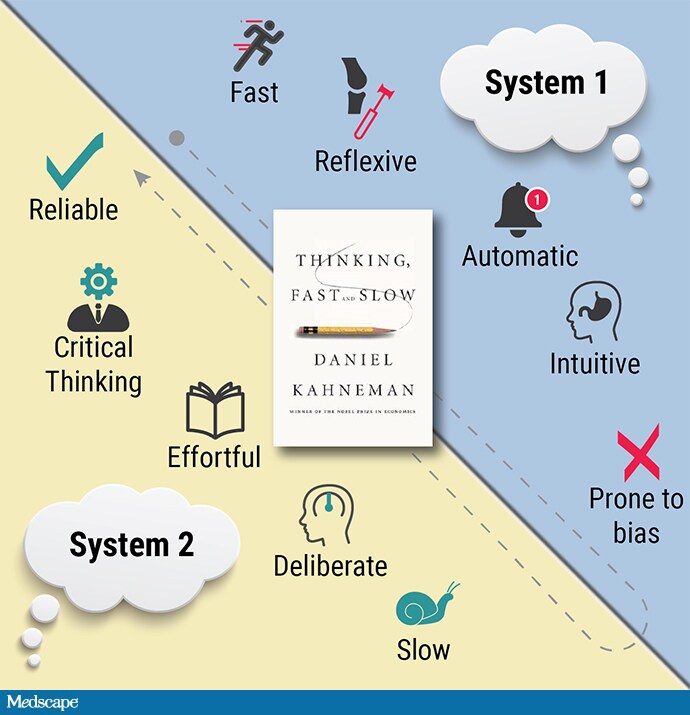
Reading Daniel Kahneman's book Thinking, Fast and Slow,[8] I realized that the vast majority of our decisions in medicine are based on system 1 thinking: fast, or reflexive, thinking. It makes us feel good and gives a sense of "doing something" for the patient. System 2 thinking is slow, analytical, effortful, and deliberate and guards against the biases of system 1 thinking. It causes significant "cognitive strain" and needs time—a rarity in the practice of modern medicine.
In managing patients with SIHD, the thought process is predominantly driven by reflexive system 1 thinking and is fraught with inherent biases. It starts with the visual model of coronary artery disease (CAD) as clogged pipes with plaque causing angina and adverse cardiovascular outcomes—a model that has been in vogue since the 1950s.[9] It is conceptually simple for physicians to use this model to explain the disease process to patients.[9,10]
If only CAD were so simple. But it is not—not even close. It is a heterogenous disease, with multiple risk factors. Patients can range from asymptomatic or symptomatic with SIHD to acute coronary syndrome (ACS) or sudden cardiac death. To date, there is no definitive way to identify the vulnerable plaque that will rupture and cause ACS.[9] Hence, focal treatment of stable plaque in patients with SIHD does not correlate to a reduction in MI or death. The pathophysiology of angina in SIHD is different from that of plaque rupture in ACS. This is a difficult concept to grasp because it runs counter to viewing all presentations of CAD through the same lens of clogged arteries.
Slow and deliberate thinking (system 2 thinking) should be cultivated to identify and overcome commonly encountered biases that Kahneman outlined in his book.[8] Here's how these biases apply to management decisions in patients with SIHD:
What you see is all there is (WYSIATI). WYSIATI is a cognitive bias where we make decisions on the basis of the information available to us and neglect what is unavailable. In patients with SIHD, any abnormality on an imaging study or stenosis on an angiogram is tangible and readily available information. PCI immediately treats the abnormality. We are easily tricked into it being a favorable option. Evidence from randomized controlled trials is counterintuitive to what we see.
Confirmation bias. The visual image of a narrowed artery now widened is a perfect set-up for confirmation bias. Physicians and patients are enthralled by images before and after PCI. In Kahneman's words, "In visual perception, you have a process that suppresses ambiguity."[11] Our minds causally translate the disappearance of the lesion into relieving angina. We believe it makes a difference, and lo and behold—patients report relief of angina immediately!
Intervention bias. This has been previously described in the practice of medicine as physicians' inclination toward recommending tests or aggressive procedures when conservative measures are equally good alternatives and medically acceptable options.[12]
All of these biases exaggerate the benefits of PCI in SIHD and corrupt the shared decision-making process.[13] Unless we recognize and acknowledge these biases, we cannot overcome them. Blinded, sham-controlled randomized trials are important in procedural fields. As an interventional cardiologist, I acknowledge the enhanced sense of satisfaction I feel after doing a PCI compared with discussing OMT with a patient. I constantly remind myself of this bias and deliberately channel my thoughts to be objective and evidence-based at every single encounter with my patients.
Optimal SIHD management needs cognitive effort and patience in addressing risk factors and uptitrating medications as tolerated. PCI is an adjunctive treatment to OMT as necessary. It is not the first-line option and cannot be done in isolation without medical therapy.
I understand the primary care physician's concerns about Mr Simon. To all those who ask about patients like Mr Simon, "If he (or she) were your family member, would you still recommend medical therapy first?" here is my firm reply: "Yes. Absolutely!"
*Some details have been changed to protect the patient's identity.
Jaya Mallidi, MD, is an interventional cardiologist at Santa Rosa Memorial Hospital in California.
Follow Jaya Mallidi on Twitter
Follow theheart.org | Medscape Cardiology on Twitter
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
© 2019 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Not so Fast: How to Avoid Bias Toward Stents in Managing SIHD - Medscape - Oct 10, 2019.










Comments