The power to predict an outcome with reliable certainty helps both providers and patients make better therapeutic choices. An area that is ripe for prediction modeling is acute kidney injury (AKI). I tend to group AKI prediction models into one of three categories: dynamic, static, and hybrid.
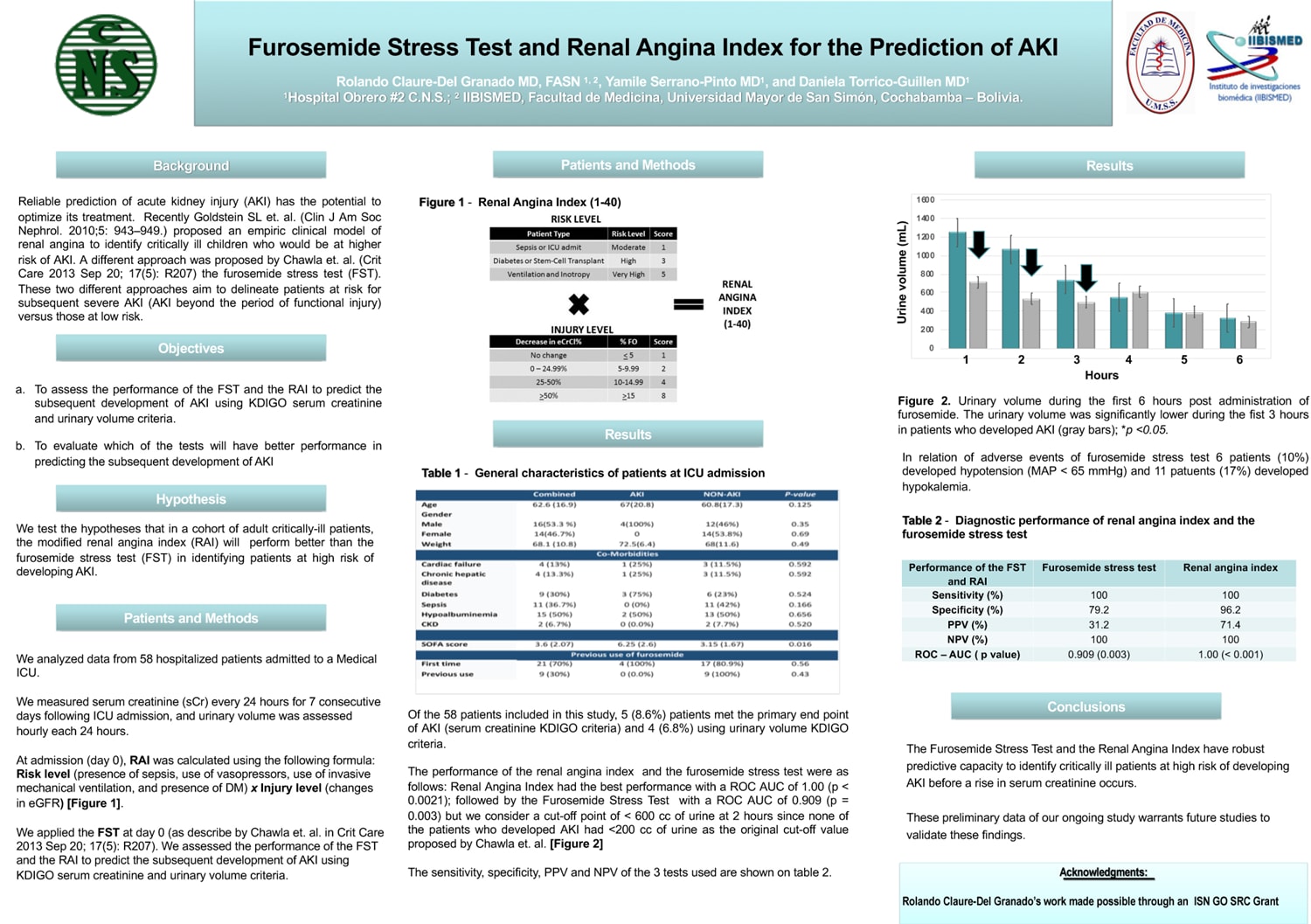
An actively researched dynamic model is the furosemide stress test. As eloquently described by Chawla and colleagues,[1] administering a moderate dose of furosemide (1.0-1.5 mg/kg body weight) to patients with mild acute kidney injury (AKIN stage 1) can identify those who will progress to severe AKI (AKIN stage 3). Patients whose urine output falls below the 200 mL threshold in the subsequent 2 hours are predicted to worsen to AKIN stage 3. While the furosemide stress test needs further validation, a number of leading-edge nephrologists from around the world recommend its use, including those in Bolivia[2,3] (see poster).

Fig. 1.
Courtesy of Rolando Claure-Del Granado, MD Download Poster
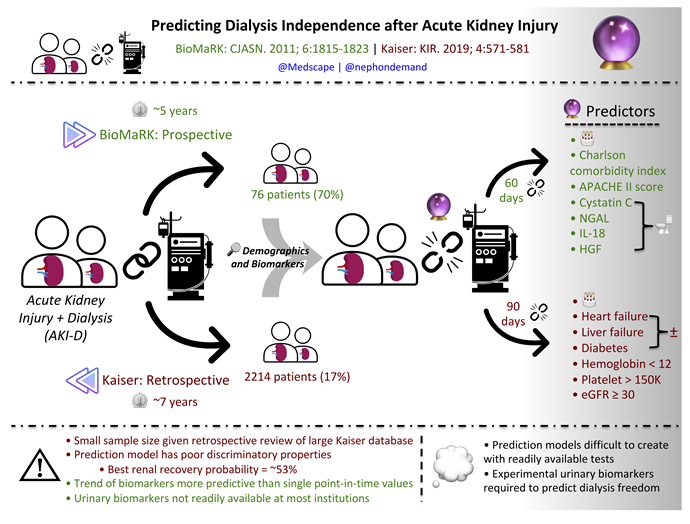
The BioMaRK model operates on the other end of the AKI spectrum. It can predict the probability of dialysis freedom in AKI patients currently receiving renal replacement therapy (AKI-D). Serial measurements of urinary biomarkers can elucidate individuals who will become free of dialysis within the next 60 days.